Travere's Filspari wins expanded approval for rare kidney disease
Travere Therapeutics secured a critical label expansion from the U.S. FDA for Filspari (sparsentan), adding Focal Segmental Glomerulosclerosis to its approved uses for reducing proteinuria. The decision widens its commercial footprint in rare kidney disease. This approval positions Filspari against a new high-need patient population with limited approved non-immunosuppressive options.
Drug Profile
Mechanism of Action Filspari (sparsentan) is a first-in-class, orally active, single-molecule antagonist of two critical pathways in kidney disease progression: the endothelin-1 (ET-1) and the angiotensin II (Ang II) pathways. It selectively blocks the endothelin A receptor (ETAR) and the angiotensin II type 1 receptor (AT1R). By inhibiting both pathways, sparsentan reduces proteinuria and provides nephroprotection through mechanisms that address inflammation, fibrosis, and podocyte injury.
Structural Differentiation Unlike a combination therapy of two separate agents—an endothelin receptor antagonist (ERA) and an angiotensin receptor blocker (ARB)—sparsentan is a single chemical entity. This design provides dual pathway blockade with a single molecule, simplifying dosing and potentially offering a distinct pharmacokinetic and pharmacodynamic profile compared to co-administering two separate drugs.
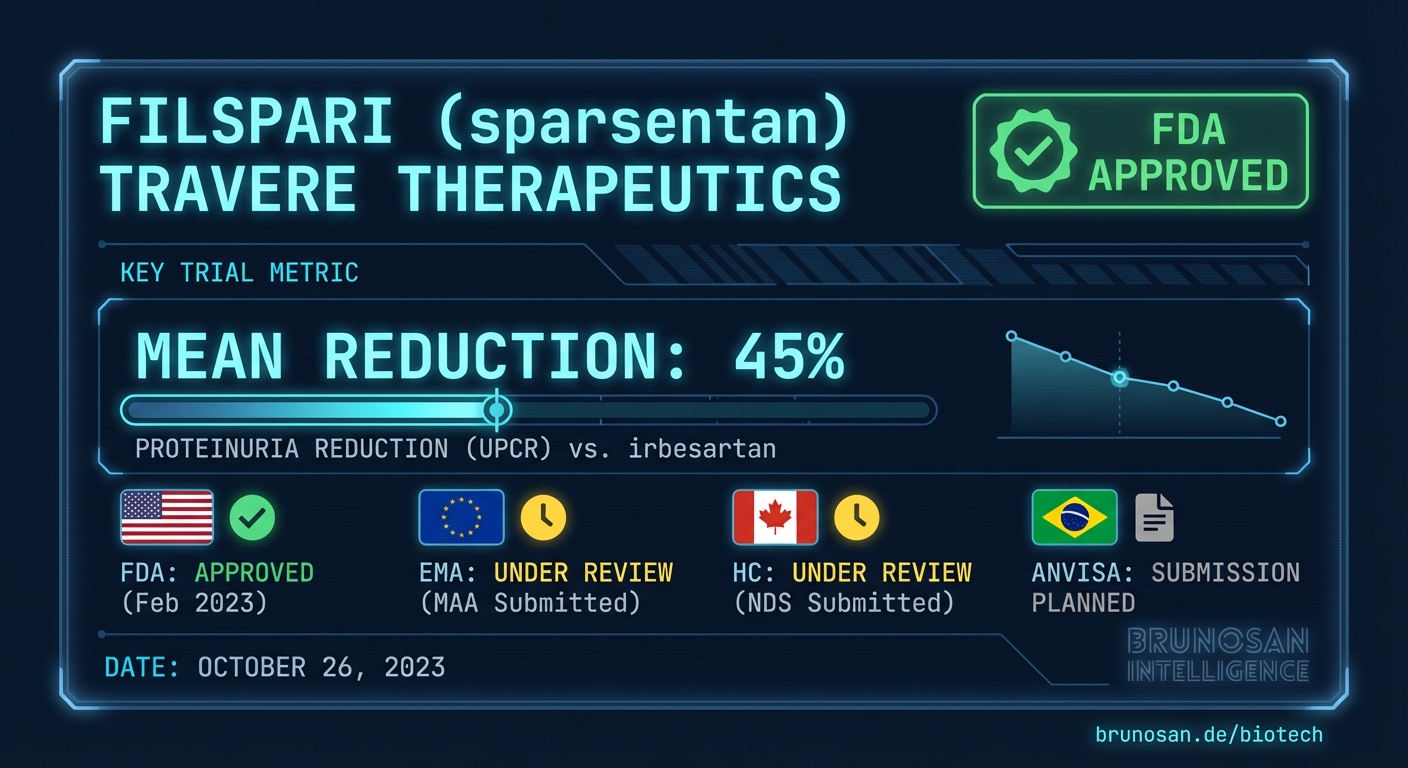
Clinical Data
The approval was supported by data from the Phase 3 DUPLEX study, which evaluated the efficacy and safety of sparsentan in patients with FSGS.
| Endpoint | Filspari (sparsentan) Result | Comparator (irbesartan) Result | Trial Name | | ---------------------------------------------- | ---------------------------- | ------------------------------ | ---------- | | FSGS Partial Remission Endpoint (FPRE) at Wk 36 | 42.0% of patients | 26.0% of patients | DUPLEX | | Mean slope of eGFR (Total) over 108 weeks | -5.8 mL/min/1.73 m² | -6.5 mL/min/1.73 m² | DUPLEX |
Global Regulatory Status
Drug-specific status across all four regulatory bodies BrunoSan tracks. Separate from pipeline volume shown in the infobar.
| Regulatory Body | Status | Notes |
|---|---|---|
| Regulatory Body | Status | |
| FDA (United States) | ✓ Approved April 15, 2026, for proteinuria reduction in FSGS. | |
| EMA (Europe) | No submission entry detected in BrunoSan DB as of 2026-04-15. | |
| Health Canada | No submission entry detected in BrunoSan DB as of 2026-04-15. | |
| ANVISA (Brazil) | No submission entry detected in BrunoSan DB as of 2026-04-15. |
STATUS
Market Impact
The FDA's decision makes Filspari the first non-immunosuppressive therapy approved for proteinuria reduction in FSGS, a rare disease that often leads to end-stage kidney disease. Prior to this approval, the standard of care involved off-label use of corticosteroids, immunosuppressants, and RAAS inhibitors like ARBs or ACE inhibitors, all with limitations in efficacy and safety. Filspari's entry provides a targeted therapeutic option that addresses two key disease pathways simultaneously. This first-mover advantage in a specific FSGS indication is substantial, allowing Travere to establish a strong foothold before potential competitors, such as pipeline assets targeting APOL1-mediated kidney disease, reach the market.
The approval carries broader implications for the nephrology sector. It reinforces the FDA's acceptance of proteinuria reduction as a surrogate endpoint reasonably likely to predict clinical benefit for accelerated approval in rare kidney diseases. This regulatory precedent lowers the development risk for other companies in the space. However, Travere's commercial success will depend on navigating payer access and demonstrating long-term value. The company's $3 billion market opportunity estimate (https://www.fiercepharma.com/pharma/landmark-fsgs-nod-hand-travere-plots-path-grabbing-filsparis-3b-us-opportunity) combines the IgAN and FSGS populations and will require effective physician education and patient identification to realize, especially as payers scrutinize the cost-benefit of new specialty drugs based on surrogate endpoint data.
Based on BrunoSan pipeline data tracking 13,803 total events, including 2,183 EMA entries and 11,276 Health Canada records, the current approval for Filspari is a U.S.-specific event. The absence of concurrent EMA or Health Canada submissions is a common strategy for rare disease assets, prioritizing the largest single market for initial commercialization before pursuing sequential global registrations. Our analysis indicates a high